The bicentenary of Florence Nightingale’s birth has coincided with the Covid-19 pandemic, and responses to the crisis have sought to build on her fame. She is lauded for having promoted hand-washing which is seen as a defence against transmission of the virus. She pioneered modern hospital design, and temporary hospitals built for the pandemic have been named after her.
Unfortunately, her most relevant work – the campaign to eliminate epidemic disease in the general population – was never publicised. As a result, the policy decisions which caused the remarkable turnaround in national average life expectancy after 1870 have been neglected in subsequent public health emergencies, including today’s.
Between 1820 and 1870 national average life expectancy in England remained at forty-one years. Outside the towns, life expectancy was increasing as it had been doing for a century. The rural improvement was being cancelled out by deteriorating life expectancy in the towns as a large proportion of the population migrated there for better wages. In 1801 only one fifth of the population had lived in towns. 50 years later it was more than half. Liverpool’s population had multiplied by nearly five, and the average life expectancy there was less than 26 years. In the largest cities half of the nation’s urban children were dying before their fifth birthday in epidemics of whooping cough, measles, scarlet fever, and diphtheria, and survivors were left with permanently impaired health.
The Poor Law Board began to take an interest in the health of the poor as it realised that epidemic disease could be an increasing cause of unemployment, poverty, and public expenditure. In 1838 the Board authorised its Secretary, Edwin Chadwick, to identify ways to reduce this expensive ill-health. He published his Report on the Sanitary Condition of the Labouring Population of Great Britain in 1842. ‘Sanitary’ had until then meant ‘relating to health’, but because Chadwick’s report identified the filthy state of the growing industrial towns as a cause of epidemic disease, his supporters began to use the word in its ‘sanitarian’ sense of cleanliness.
Chadwick’s first contribution to the fight against epidemics had been his suggestion of recording the cause of death when the compulsory national registration of births and deaths began in 1837. He proposed the radical physician and journalist Dr William Farr as ‘compiler of abstracts’ in the Registrar-General’s Office at Somerset House. Farr’s statistical and literary abilities were to prove invaluable in mining the registration database.
Chadwick believed, like most medical practitioners in the 1830s, in the miasma theory that epidemic disease was propagated by ‘atmospheric impurities produced by decomposing animal and vegetable substances, by damp and filth, and close and overcrowded dwelling’. The lack of ventilation in the homes of the poor, he believed, exacerbated the action of the polluted environment. His proposed solution was to remove the filth from dwellings and streets by means of sewer pipes continuously flushed with water.
Chadwick’s work led to the 1848 Public Health Act which set up a General Board of Health with Chadwick as Commissioner. However, the 1848 Act was ‘permissive’: a minority of voters could opt their locality into the oversight of the General Board of Health. A newspaper campaign accused Chadwick and the Board of ‘centralisation’, a code word for attacking the vested interests of local property owners. When Parliament debated a prolongation of the Board in 1854, Chadwick could not muster enough personal support. The Board survived in restructured form, but Chadwick was obliged to retire from the Civil Service at the age of 54.
After Chadwick’s departure, the General Board of Health appointed the surgeon and pathologist John Simon as its Chief Medical Officer. Simon was careful not to be as coercive as Chadwick in enforcing existing legislation which would provoke reaction from property interests that would imperil his medical work.
Simon saw his role as developing a comprehensive state medicine which would cure or prevent specific epidemic diseases after identifying their causes. At a time when germ theory was a vague etiological hypothesis, alongside such alternatives as electricity in the atmosphere, bad smells, or damp ground, Simon’s technocratic vision was futuristic. It could also blind him to sanitarian solutions that would improve clinical outcomes without identifying specific diseases and their causes. For example, in his 1858 official report he poured cold water on what he called Dr John Snow’s ‘peculiar doctrine’ that cholera could be transmitted through contaminated drinking water.
Despite the exalted, almost dictatorial, powers conferred on Chadwick and then Simon by the Public Health Act of 1848, there was no improvement in national life expectancy during the period from 1840 through to the 1870s. Parliament had tried two radically different approaches to the economic problems caused by epidemic disease: infrastructure planning and medical research. Both relied on highly centralised control.
Florence Nightingale became involved with the sanitarian campaign in 1858 out of dissatisfaction with the treatment of common soldiers during the Crimean War. After returning from the Crimea in the summer of 1856, she worked intensively with William Farr on the statistics of deaths from sickness during the war. They concluded that sanitary defects in the hospitals had caused the high mortality of the Crimean army from sickness.
From Farr, Nightingale learned about Chadwick’s unconventional sewage removal designs involving running water and glazed earthenware pipes. In the report she wrote for the Minister of War, she laid the blame for the excessive army mortality on neglect of Chadwick’s doctrine of ventilation, drainage, and reduced overcrowding: “The operative causes of our great mortality were - 1. Overcrowding of the Patients in the buildings... 2. Extremely defective drainage.”
Nightingale attacked John Simon, the Chief Medical Officer, in print for claiming that deaths from whooping cough, measles, and scarlet fever could not be prevented. A long exchange in the specialist press between Nightingale and Simon and his colleagues established that the Chief Medical Officer was not aware that improved ventilation could reduce mortality from these diseases even if it could not prevent their incidence. This had been one of Chadwick’s beliefs. She showed that Simon was also unaware of Farr’s discovery that death from these airborne diseases was more likely if the victim had previously suffered from enteric disease caught from sewage. The effect of this controversy was to bring Chadwick onto Nightingale’s side; until then he had regarded Simon as a fellow-sanitarian. He and Nightingale now joined forces to undermine the Chief Medical Officer. Farr, a lowly civil servant despite his exceptional talents, remained more conciliatory towards Simon although he was happy to provide sanitarian ammunition.
Nightingale made the relaunch of Chadwick’s movement her priority, distancing herself from the hospital work that had made her famous. Her written output over the next decades was prodigious, and she constantly promoted Chadwick’s ideas on ventilation and drainage. She leaked copies of her confidential report to the Minister of War, sending it to the most influential people under seal of confidentiality. She wrote for every level of society, from parliamentarians, royalty, and scientists to domestic servants. Her most famous and popular book, Notes on Nursing, (1860, suggested to her by Chadwick) was more about domestic hygiene than hands-on patient care, and introduced the concept of ‘health of houses’ which depended on “Pure air, pure water, efficient drainage, cleanliness and light”. She organised ‘health missioners’ and district nurses to spread the message by word of mouth to a less literate audience, on occasion poaching hospital nurses from the Nightingale Fund training school at St. Thomas’s for the purpose. Her reputation among the working-class families whose sons had died in their thousands during the Crimean War, her social standing, her communication skills, and the tacit support provided by a constellation of liberal-minded politicians, enabled her to convince people from all classes of the need for better hygiene.
When a Royal Sanitary Commission drafted legislation in 1871 requiring all new houses to connect to mains drainage, Nightingale asked James Stansfeld, ministerial President of the new Local Government Board, to amend the Bill to include existing houses. She also suggested giving inspectors the right to check internal drainage and water supply arrangements as well as external connections. It was done, with the Minister quoting her almost word-for-word in the Commons to justify his amendments. Meanwhile, she and Chadwick suggested that Stansfeld deprive the Chief Medical Officer of his centralised power of enforcement. The Minister duly devolved enforcement to local authorities. Medical responsibilities now rested with local Medical Officers of Health, who were less interested in leading-edge medical research than John Simon and his colleagues and more concerned with immediate practical solutions.
The Nightingale-inspired legislation received Royal Assent as the 1875 Public Health Act. From that date onward, national life expectancy rose steadily, increasing by half before medical science had anything to contribute to the prevention or cure of the principle epidemic diseases (Figure 1).
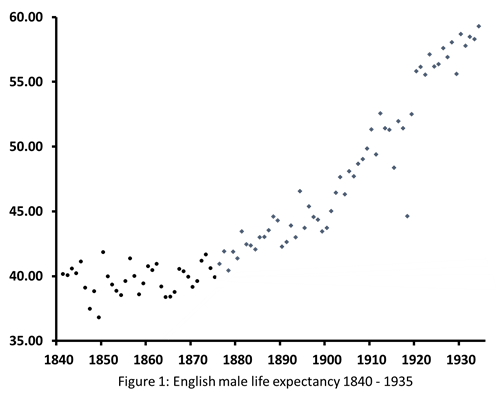
Source: Office for National Statistics
The censorship in Nightingale’s official biographies obscured her contribution to the nation’s improving health after 1870. Consequently, there has been no satisfactory explanation of why the entrenched popular opposition to compulsory sanitation melted away between 1854 and 1871.
The scientific contributions of Chadwick and Farr were lost to medical and public health practice for a century and a half. This loss is evident in the World Health Report of 1996: Fighting Disease, Fostering Development. The report showed that infectious disease was the world’s major cause of death in 1996, accounting for one third of all deaths in the developing world just as it did in 1840’s England.
WHO identified bacterial pneumonia as the main killer among its list of diseases ‘transmitted from person to person.’ The report stated that only children who had previously been weakened by other infections were falling ill as a result of acquiring it, but did not identify the other infections which cause the delayed death of children when they catch the common pneumonia bacterium. The culprits must include diarrhoea, transmitted by defective sanitation, which was by far the most common childhood infection according to WHO’s statistics. WHO did not try to calculate how many of the eleven million annual deaths listed as being caused by diseases ‘transmitted from person to person’ – one fifth of all deaths in the world – could be prevented by improved sanitation.
The WHO system of disease classification aimed at counting the deaths that could be avoided by battling against infections, and in so doing obscured the number of lives that would be saved by improving sanitation and making infections harmless. In its conclusions, the WHO report fell victim to the illusion thus created that curative medicine was the only solution:
WHO has set the target of reducing deaths from acute respiratory infections [largely pneumonia] in children under age 5 by one-third by the year 2000 – equal to more than 1.4 million lives saved per year. But achieving this target is threatened because, as mentioned earlier, the two cheapest and hitherto best antibiotics to treat pneumonia, the leading killer among acute respiratory infections, are now much less effective due to bacterial resistance. This means that either more expensive drugs must be used, or that more children will die from these infections.
The last sentence states categorically and erroneously that drugs alone can prevent these deaths, implying that improving sanitation or reducing overcrowding can play no role. It is the same mistake made by England’s Chief Medical Officer in 1858 and by historians since.
National medical leadership had to be removed from decision-making before the 1871-75 Acts could resolve the problem of epidemic disease. The medical expertise of those days was negligible compared to recent times. But despite this progress, medical practitioners can still be insensitive to the special requirements of public health, as shown by the WHO example quoted. In another example, ‘prevention’ to a medical practitioner tends to refer to prevention of disease rather than prevention of permanent harm to the patient resulting from the disease. This still leads to misunderstandings between medical and public health experts.
It is therefore troubling that in Britain the two principal government advisers chosen during the Covid-19 public health crisis (Chief Medical Officer and Chief Scientist) were both medical practitioners. They gave ‘scientific’ advice on subjects unrelated to their area of expertise. For example, the Chief Medical Officer advised delaying compulsory social distancing measures, saying “There is a risk if we go too early people will understandably get fatigued and it will be difficult to sustain this over time.” This was on 9 March 2020, two weeks before the government imposed lockdown measures, on the day that the fifth person died in Britain after testing positive for the virus. When challenged on the issue of whether the government was moving too slowly, the Prime Minister implied that the Chief Medical Officer’s opinion was scientific: “… it is vital that we take the steps that we think are necessary at the right time and we follow the science.” No evidence was given of supposed ‘lockdown fatigue’. On 14 March, 200 academic scientists from a variety of disciplines wrote an open letter criticising the delay and calling for ‘additional and more restrictive’ social distancing measures.
Politicians tend to be educated in the humanities rather than science, and it would not be surprising if they regard medical practitioners as the “go to” scientists. It is also possible, when medical practitioners are faced with issues outside their specialist areas, that they hesitate to endorse measures that would impose an apparent economic burden. This may help to explain why the Chief Medical Officer in 1858 was reluctant to enforce sanitary legislation, and why WHO doctors in 1996 ignored the sanitary option.
As a thought experiment, one might imagine what would be the outcome if the 200 concerned scientists were each asked to choose two scientific adviser profiles to deal with a pandemic infection and the results were averaged out in the ‘wisdom of crowds’ approach. It seems unlikely that a pair of medical practitioners would have emerged as the top advisory team.
A major fuel that powered the rollout of the lifesaving water and sewer infrastructure after 1870 was local annual property tax. Annual taxes on property values, or ‘rates’, had been used since medieval times, starting with the ‘poor rate’ to care for the indigent. Other taxes on property owners, such as a ‘highway rate’ were also used. The tax was proportional to individual property value, so if property values increased then so did the tax yield. From the 1870s Local Authorities were allowed to levy annual property tax to fund the installation of compulsory mains drainage, borrowing capital on the security of their tax base. Those Authorities who tried it found that mains drainage could directly increase the value of the properties that paid the tax. This created a virtuous circle that benefited landlords financially as well as increasing the tax yield and improving the health of all residents.
Elected Local Authorities had now discovered the tax that makes the taxpayers richer as well as energising cooperation between citizens of all classes to improve their locality. Then, as now, an important factor driving up property prices was improvement in the public realm. Other local services also developed using the same financing mechanism until by 1905 more than half of all national public expenditure was by self-financing Local Authorities.
Annual property taxes based on regular revaluation of individual properties is widely used internationally (including the British Commonwealth) for improving the local public realm (and hence private property values), but no longer in Britain. Paradoxically, although Council Tax receipts are higher than the local property taxes in most other countries, central government’s design of Council Tax renders it incapable of serving that purpose. It is hugely regressive, with the lowest value properties paying more than five times as much as the highest, and no revaluation takes place so that increasing property values have no impact on tax yield. Often the demise of the Victorian system in Britain is blamed on the Conservative government’s abolition of the domestic rate in 1990, or on the Labour government’s failure to restore it when they came to power. But these were only milestones in the long non-partisan process of downgrading elected Local Authorities and hoarding power for central government. As Travers and Esposito have shown, the process began in the 1920’s and will continue as long as Britain’s malleable constitution allows electoral democracy to be an unconstrained quest for absolute power.
All independent experts have recommended a return to the gold standard of annual ad valorem property taxes with regular revaluations, including the Institute for Fiscal Studies Mirrlees Review. There is no suggestion that the overall tax bill for UK taxpayers should increase. Britain is already in the top three countries in the OECD for property tax. Much of it goes to central government as Stamp Duty Land Tax payable on property purchase, a tax which nearly all comes from central London boroughs with sky-high property prices and which impedes nationwide labour mobility. Abolishing SDLT and Council Tax and reducing the counterproductive and inefficient taxes on labour will reduce the overall tax burden. The losers will be foreign investors who pay no UK income tax and would find themselves paying as much tax as they do in other countries where they invest in property.
The peculiar centralisation of fiscal policy will have to end if the UK is to control future pandemics, repurpose urban assets, and mobilise a new economy.
The Covid-19 pandemic has placed new strains on the relationship between central government and subordinate Local Authorities which have been reduced to ‘branch offices of Whitehall’ in the memorable phrase of Conservative politician Michel Heseltine. The national centralised test-and-trace system is failing to find a significant number of contacts identified by people who have tested positive for the virus. This failure exposes shortcomings which can only be resolved by local action. Suspected carriers of the virus, particularly in deprived areas, are often unwilling to be contacted by telephone and told that they and their families must stop working and self-isolate. Language difficulties are another barrier. Some Local Authorities in badly-hit areas have set up their own track-and-trace systems relying on home visits by staff equipped to offer support. After petitioning central government, these authorities are now allowed access to infection records, and central government has seconded staff to work with them. It is arguable that central government should never have attempted to trace infection suspects using a central database. Local Authorities with their extensive data on local families, communities, and geography are clearly better equipped, as they demonstrated in Victorian times.
Restructuring government finance and devolving key functions, as outlined above, is not just about the response to the immediate crisis. Local authorities will also inevitably play a role in reconstructing local economies and facilitating new behaviour after the Covid-19 pandemic. The pandemic has disrupted travel, office work, education, and bricks-and-mortar retailing and brought the national economy to a virtual standstill. The sudden collapse of these sectors has exposed systemic weaknesses and technical obsolescence which were already reducing their fitness for purpose or causing their rapid decline. Mass transit systems were inefficiently sized for diurnal rush-hours. The hidden costs of commuting were becoming apparent: chronic stress, road danger, and house price inflation. It must not be forgotten that we were already in the middle of the ‘inactivity pandemic’ when Covid-19 struck, and were studying how to repurpose our urban areas to improve the ‘health of streets’, the modern equivalent of Nightingale’s ‘health of houses’. Efficient and convenient travel is the proximate cause of the Covid-19 pandemic, just as human effluent caused the great epidemics. Like travel, effluent was a profitable industry in its own right: ‘night soil men’ traded and stockpiled ordure for use as manure, the role of houseflies as vectors of disease being not yet recognised.
Before the online shopping boom arrived our urban centres were already over-equipped with retail premises at the expense of their traditional community role. Since the 1970s Local Authority planners had been competing self-destructively against each other to attract the newly-motorised shopper from out of town. Our town centres were broken, and must be repaired. Repurposing to their original community role, with local shops more accessible by active travel, will prevent future pandemic transmission and at the same time improve the wellbeing of the urban population.
It is hard to see how the necessary changes of use can be planned without intensive work by Local Authorities who have the necessary information at their fingertips. The elimination of epidemics between 1875 and 1955 required rebuilding a large proportion of the national urban housing stock. As then, with careful local planning, adequate financing, and compulsory purchase the result will be economically profitable.
The social revolution of the 1870s was only possible because the behaviour of the population had been changed by a decade and a half of sanitarian propaganda. In modern times the consumer electronics industry has demonstrated how to rapidly change social behaviour. The pandemic will spur the industry to convert the population from the small screen to the wall-screen, possibly in local centres where people can work and study as well as socialise in person with members of their own community rather than with schoolmates or workmates. It will be unfortunate if governments urge the population to go back to the office and relaunch the city centre economy, in competition with the ‘tech giants’ who are working to popularise home working.
A property tax administered at local level is also the best way to finance rapid regrowth of the economy. Central government likes to aim for increases in GDP although, as the Office for Budgetary Responsibility reminded the Prime Minister in 2013, its austerity measures have limited GDP growth. Centrally-promoted megaprojects like hub airport expansion, the channel tunnel, Crossrail, nuclear power stations, and HS2 increase headline GDP in the years of construction. They propose a profitable return on capital beginning decades in the future based on calculations which may be impossible to verify when the time comes. If the return does not materialise an opportunity cost is incurred because the capital could have been used for a more productive investment.
The government’s recent change to planning rules allowing two-storey home extensions without planning permission seems to be similarly destined to create a short-term construction boom rather than long-term economic growth. It may well increase the value of the properties concerned while reducing the value of neighbouring properties.
Local government can borrow at most advantageous rates for improvements to the public realm where, in contrast, the return is more immediate and measurable in terms of increased property tax yield and improvements in housing. Some oversight by central government is needed to avoid wasteful competition between communities, to equalise between areas, and to resolve other issues. The advantage of using the world-standard property tax is that experience in other countries can be exploited to identify appropriate mechanisms.
The obvious way forward is to incorporate into law the European Charter of Local Self-Government, an international treaty ratified by the UK in 1998 as a member of the Council of Europe to which the country still belongs. A bill before the Holyrood parliament already aims to do this for Scotland.
Widespread epidemic disease in mid-Victorian Britain was as economically and socially disruptive as the Covid-19 pandemic today. The turning point came in the 1870s when the focus changed from medical intervention to behavioural change and practical public health measures under the control of self-financing Local Authorities.
Failure to heed the lessons of the 1870s has hindered responses to other public health crises including the current pandemic. In rebuilding the economy after the pandemic, too, the post-1870 urban reconstruction programme needs to be a model for repurposing the national infrastructure.
It is a dramatic irony that in her bicentenary year the misrepresentation of the principal enabler of the late Victorian public health revolution, Florence Nightingale, has perpetuated ignorance of past successes. The hospital-centric portrayal of the sanitary activist has encouraged complacency in the face of excessively medicalising approaches to the current crisis.
Bogdanor, V. A New Localism? In The New British Constitution. Hart, Oxford, 2009.
Small, H. Edwin Chadwick: a Biographical Update. Journal of Medical Biography (in press: https://doi.org/10.1177/0967772020951083.)
Small, H. Florence Nightingale and Her Real Legacy: A Public Health Revolution. London, Robinson 2017.
Travers, T. and Esposito, L. The Decline and Fall of Local Democracy: A History of Local Government Finance

Sign up to receive announcements on events, the latest research and more!
We will never send spam and you can unsubscribe any time.
H&P is based at the Institute of Historical Research, Senate House, University of London.
We are the only project in the UK providing access to an international network of more than 500 historians with a broad range of expertise. H&P offers a range of resources for historians, policy makers and journalists.